
What is an ACO and what do you need to know about them?
by Michael Jones
If you are a primary care practice, you’ve likely been approached within the last few weeks about joining an Accountable Care Organization (ACO), possibly by multiple different groups. The reason for this flurry of activity is Phase 1 of the ACO application program goes from May 18 to June 15, 2023 and the final phase to add TINs to an ACO is July 11 to August 1, 2023. If you’re not already in an ACO, you’ll need to make some important decisions about whether or not to join an ACO for 2024, and which ACO to join.
Before you commit to joining an ACO, you should take time to educate yourself through multiple sources, with your main source being CMS.
You can find several resources directly from CMS here:
Specifically the Current Years Shared Savings and Losses and Assignment Methodology Specifications section (current version is Version 10, which can be found here: SHARED SAVINGS AND LOSSES AND ASSIGNMENT METHODOLOGY Version 10
According to CMS at https://www.cms.gov/medicare/medicare-fee-for-service-payment/aco:
“ACOs are groups of doctors, hospitals, and other health care providers, who come together voluntarily to give coordinated high-quality care to their Medicare patients.”
“The goal of coordinated care is to ensure that patients get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors.”
“When an ACO succeeds both in delivering high-quality care and spending health care dollars more wisely, the ACO will share in the savings it achieves for the Medicare program.”
The goal of the ACO, again according to CMS, is to:
Promote accountability for a patient population
Coordinate items and services for Medicare Fee For Service beneficiaries (as opposed to beneficiaries in a Medicare Advantage or qualified retirement plan)
Encourage investment in high quality and efficient services
This is a voluntary program that rewards participating physician practices for achieving cost savings of an assigned pool of Medicare beneficiaries during a calendar year compared to the baseline geographically adjusted cost benchmark. CMS and CMMI have already shared their intent for all Medicare fee for service beneficiaries to be in a care relationship with accountability for quality and total cost of care by 2030 in their 2022 strategic direction whitepaper, and enrollment in the 2023 calendar year will be for performance year 2024, from January 1 through December 31, 2024.
Prior to the ACO Reach model, the ACO shared savings participation options are shown below, from a prior year document titled Shared Savings Program Participation Options for Performance Year 2023 (this information is still valid for performance year 2024, with the addition of the ACO Reach program.
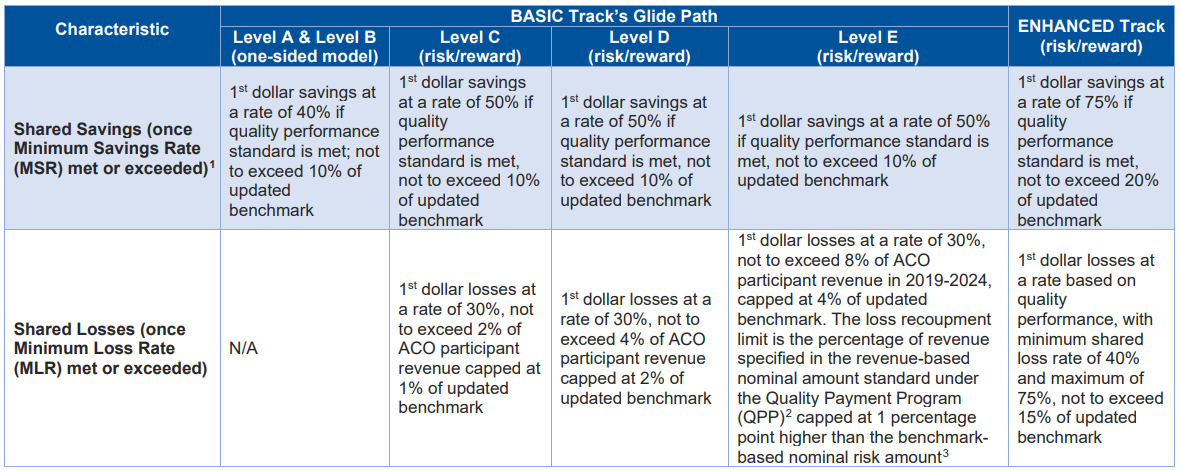
The further along the tracks listed above, the greater both the reward and the risk. In the one-sided model Level A and Level B, for example, there is no shared losses as part of the ACO model, but first dollar shared savings are at a rate of 40%, compared to Level C, which includes a shared loss component, and first dollar shared savings at a rate of 50%. The further along the risk spectrum, the greater the reward, with the culmination being the Enhanced Track, which has the greatest reward and the highest risk. This track is typically for more advanced groups who have a full understanding of and system for tracking costs and patient data.
Your most valuable CMS resource in understand the ACO program is the current SHARED SAVINGS AND LOSSES AND ASSIGNMENT METHODOLOGY document. First, check to make sure that you are viewing the most current version of this document, as these handbooks change periodically. CMS is currently on Version 10, which you can verify at the Programs & Guidance page listed earlier.
This document is a 74 page manual that gives you a detailed description of the following areas:
Assignment of beneficiaries
ACO per capita expenditures, risk adjustment and ACO participants’ revenue
Shared savings and losses calculations
Multiple appendices and ACO abbreviations and key terms
The opening line of this document states that “this document is not intended to supersede or replace regulatory requirements under 42 CFR part 425”, which can be found here.
As you can see, there is a mountain of information on what the Accountable Care Organization program is as well as how the program has performed historically, both on the whole and at the single, specific ACO level. The key to understanding and making the decision to join an ACO is that the program offers physicians the opportunity to earn additional revenue, in exchange for being held accountable for the “quality, cost, and experience of care” of assigned Medicare beneficiaries.
At the most simplistic level, an ACO is assigned a weighted cost per beneficiary, based on several years of historical cost information. When the ACO outperforms this benchmark during the performance year, with regional adjustments, the ACO shares in the additional incremental savings with CMS.
There is much more to the program, including the newly added ACO Reach model, which we will explore in more depth over the next several weeks.
